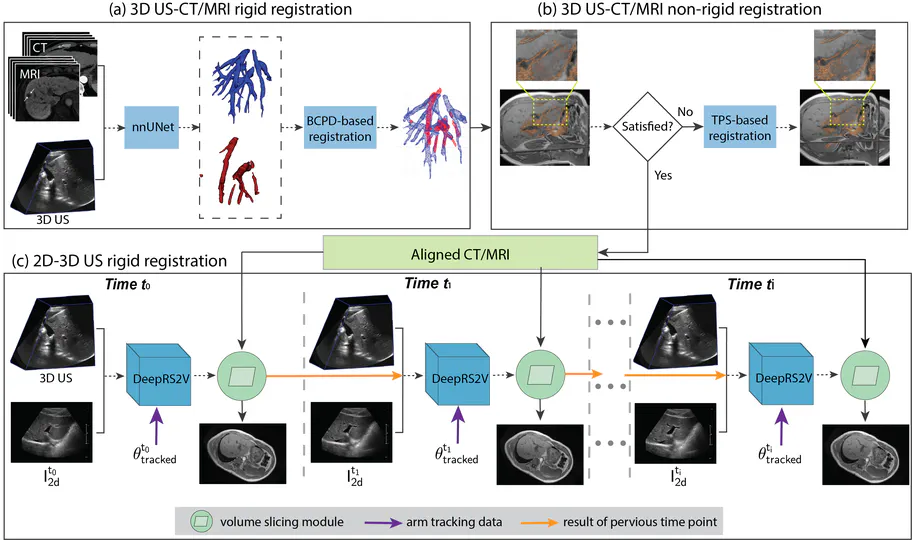
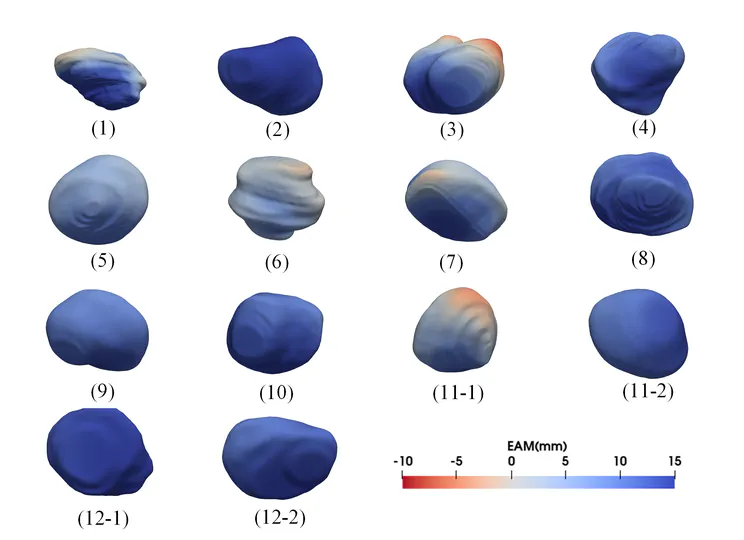
Project 1: US-guided Percutaneous Liver Tumor Ablation
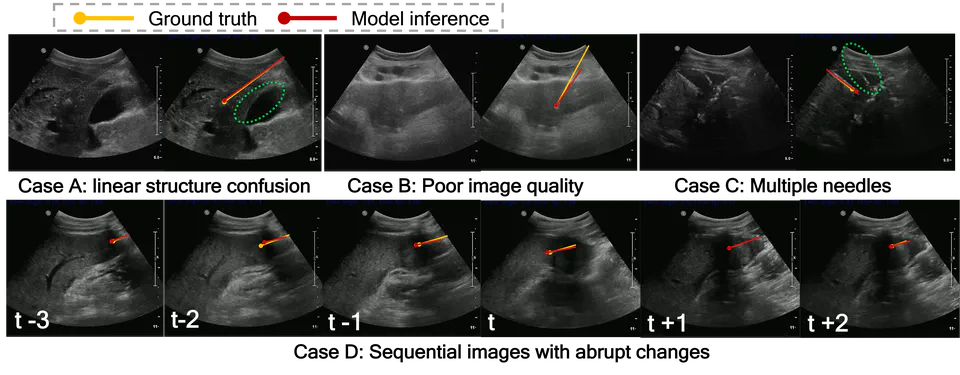
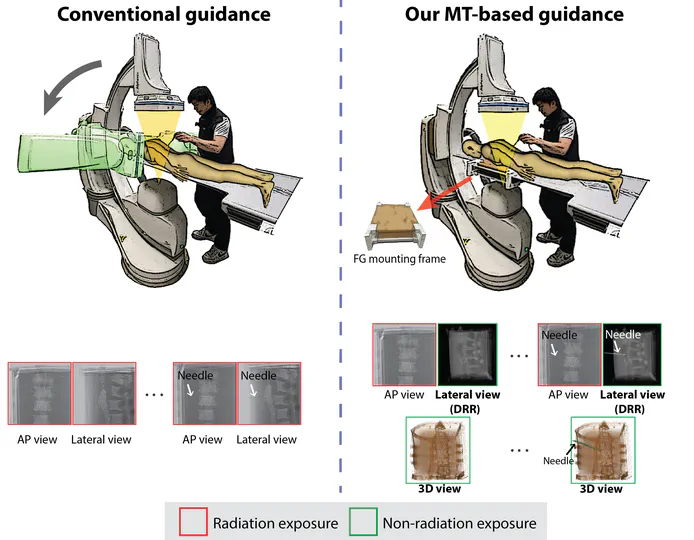
Project 2: Integration of Magnetic Tracking into Fluoroscopy-guided Interventions
In collaboration with Northern Digital Inc. (NDI), I contributed to pioneering the integration of magnetic tracking into fluoroscopy-guided interventions.